
Proactive Narcotic Abuse Screening
Case: An independent pharmacy filling high-doses of narcotic CNS depressants for a middle-aged man, receives notice of a claim. The patient was found unresponsive by his wife, and pronounced dead at the scene. Toxicology reports indicate supratherapeutic concentrations of hydrocodone, oxycodone, and alprazolam. Additionally, multiple tablets of Oxycontin® are found in the patient’s stomach upon autopsy. Looking through the patient’s record, it is noted that the patient paid cash on multiple occasions for early fills of the same medications. The pharmacy claims the patient’s reason for the early fills includes ‘vacation-supply’ and ‘lost-supply’. The prescriptions were written by a variety of physicians in different practices, and no effort was made to confirm their knowledge of the other’s care. Additionally, records revealed prescriptions were also filled at other pharmacies in the area.
Result: The filling pharmacist was found liable, resulting in over $200,000 paid out in liability and litigation fees.
The Centers for Disease Control and Prevention (CDC) has declared prescription drug abuse an epidemic, with prescription opioid overdose deaths outnumbering heroin and cocaine overdose deaths combined1. In 2011, 16,917 drug poisoning deaths involved an opioid analgesic, which is more than quadrupled from 19992. According to the National Survey on Drug Use and Health, over 14 million individuals aged 12 or older used prescription drugs nonmedically in the past 12 months3. The increased incidence of prescription drug abuse and related overdose is both alarming and actionable.
Healthcare providers are the gatekeepers of patient access to prescription drugs. When a patient’s addiction takes hold, those gatekeepers must intervene. Community pharmacists are optimally positioned to ensure the appropriate use of controlled substances. When a patient presents to the pharmacy with a prescription for a controlled substance, the following questions should be addressed:
- Has the patient filled here before?
- Does it logistically make sense for the patient to be filling their medication here? (i.e. How far away is their home address and/or doctor’s office from the pharmacy?)
- Is the patient filling this prescription through insurance?
- If a patient’s medication history is available, is there only one physician/ practice prescribing controlled substances for this patient?
- Is this prescription being filled early?
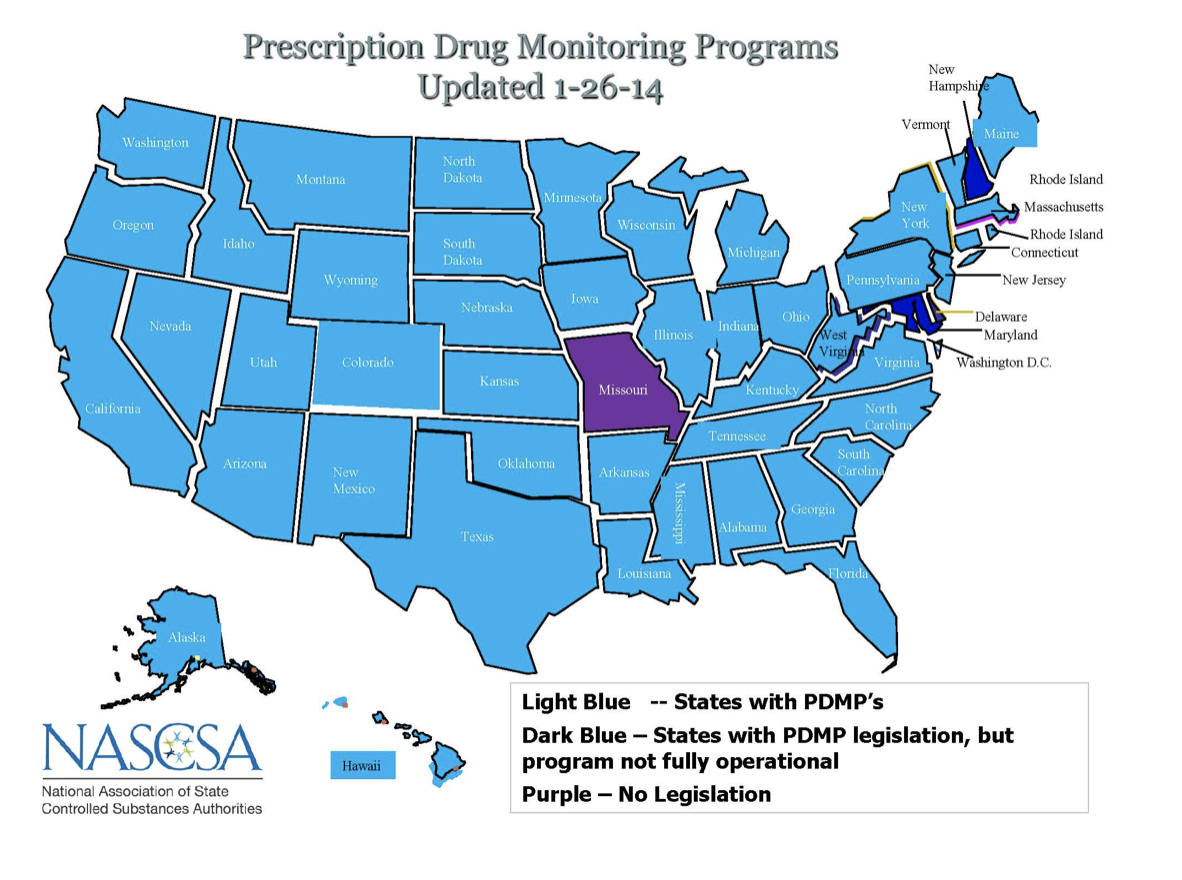
Answering ‘no’ to any one of the above questions warrants further investigation into the prescription’s legitimacy. Prescription Drug Monitoring Programs (PDMPs) are an excellent resource that should be utilized to ensure appropriate drug therapy. Currently, 49 of 50 states (all except Missouri) have PDMPs, while some are not fully operational (Figure 1). Further information regarding the PDMP in your state can be found on the National Association of State Controlled Substance Authorities’ website (http://www.nascsa.org/stateprofiles.htm). Checking the PDMP, contacting the prescribing physician(s), and determining the drug’s indication are prudent ways to mitigate the risk of filling a prescription which may be potentially abused. Any information regarding the appropriateness of therapy should always be documented.
Prescription drug abuse is a public health problem that deserves special attention. Instating proactive measures to ensure appropriate drug therapy in regards to controlled substances is of utmost importance given the breadth of the problem. This will in turn reduce potential claims of liability and improve your pharmacy practice. Most importantly, it will further enable pharmacists to advocate for their most vulnerable patients.
 — Edward R. King, Pharmacy Student Intern
— Edward R. King, Pharmacy Student Intern
For more information, reference sources are available on request. If you need to contact Eddy King, please let us know at risk.mgmt@phmic.com.